Self-Care as an Ethical Principle: A Pre- and Post-Pandemic Onset Integrative Review of COVID-19
Marta Luciane Fischer1
*
 and Tuany Anna Maciel Burda2
and Tuany Anna Maciel Burda2
1
Bioethics Master Program at Pontifice University Paraná,
Brazil, R. Imac. Conceição,
Prado Velho,
Curitiba- PR
Brazil
2
Bioethics at the Postgraduate Program in Bioethics at PUCPR,
Brazil. R. Imac. Conceição,
Prado Velho,
Curitiba - PR
Brazil
http://dx.doi.org/10.12944/CWE.18.1.4
Copy the following to cite this article:
Fischer M. L, Burda T. A. M. Self-Care as an Ethical Principle: A Pre- and Post-Pandemic Onset Integrative Review of COVID-19. Curr World Environ 2023;18(1). DOI:http://dx.doi.org/10.12944/CWE.18.1.4
Copy the following to cite this URL:
Fischer M. L, Burda T. A. M. Self-Care as an Ethical Principle: A Pre- and Post-Pandemic Onset Integrative Review of COVID-19. Curr World Environ 2023;18(1).
Download article (pdf) Citation Manager Publish History

Introduction
Self-care is understood and widely applied as voluntary actions resulting from deliberate, reflective judgments, and leading to appropriate actions through definition, direction, and behavioral regulation.1 According to Orem1, it constitutes a universal requirement of the fulfillment of basic human needs. The term has established itself in the field of nursing, based on the understanding that the role of nursing professionals is to assist in self-care through orientation and education.2
Self-care centers on the totality paradigm, wherein the individual needs to adapt to the multidimensional environment by contemplating biological, psychological, social, and spiritual aspects.2 Orem1 considered self-care to be a holistic approach to the health and care of human beings, a set of activities and actions acquired over a lifetime, undergoing variations based on beliefs, habits, customs, and culture. Therefore, it is an individual’s continuously constructed practice for themselves wherein they assume the role of the agent of their care. Tobón-Correa3 suggested that self-care as a simultaneously individual, collective, theoretical, and practical act that can be planned and developed in cooperation with the physical, social, emotional, and supportive environment, to reestablish health and prevent disease, is a philosophy of life permanently strengthened through self-awareness, self-control, self-esteem, self-acceptance, and resilience. According to Palodeto and Fischer4, self-care should be conceived as an ethical, respectful conduct with oneself and others, which is conditioned by self-awareness and involvement with all the processes included in the acquisition, remediation, and prevention of health problems. These authors assessed self-care within the context of the conscious use of medication, calling for a reframing of the health-disease paradigm, and commitment to decisions associated with the processes of research, production, distribution, and disposal of medication. Palodeto and Fischer5, evaluating the social representation of medication and identifying a global view of health, warned that specificities evidence a relationship between self-perception and self-management of health. Research supports the confluence between bioethics and global health for promoting ethical and educational discussions as well as self-care and environmental-care to prevent diseases and uphold the health and quality of life for humans and ecosystems at the local level, with global repercussions, benefitting present and future generations.
The commitment to self-care from a global health perspective involves the dimensions of body/mind/spirit, individual/collective/nature, and local/global, becoming especially apparent in experiences with pandemics. 6,7,8,9 This can be seen in the case of coronavirus disease (COVID-19), which has stirred a debate about the need for self-care as a measure to contain infections and suddenly determined a change in people’s habits around the world. This perspective includes environmental bioethics, with its dialogical and multidisciplinary nature, lending itself to consider the needs, interests, and values ??of the moral agents involved in an ethical issue and guiding to a consensual, fair solution based on common values ??that transcend local space and time.6,7 Therefore, self-care can be related to an ethical behavior of self-responsibility and collective responsibility as it involves commitment to the other.5,10
Based on the premise that self-care turns one into a healthy person capable of establishing quality relationships, in the expectation of equitable exchanges, when exercising self-care, people look at themselves, others, and the environment. Thus, the problem of this research questions how the self-care terminology has been defined, understood, and applied in the scientific and popular context. The relevance of this study is based on the expectative that knowledge of different conceptions, will be possible to invest in educational interventions to promote global health in formal education10 and in spaces collective, as social media, that promotes education by means sharing of individual experiences.9 This study also aims to test the hypothesis that there are differences in the conception of self-care between the scientific and non-scientific communities, the Brazilian and international communities, and before and after the COVID-19 pandemic.
Methods
This is a cross-sectional mixed methods study based on an integrative review11, and it explores how the scientific and non-scientific communities have approached self-care.
Scientific conception
The first stage of the study consisted of an integrative review based on scientific knowledge, where we used Google Scholar and databases: SciELO, DOAJ, MEDLINE, Bioline). For each tool, we considered as inclusion criteria the first 100 suggestions for the term “autocuidado” (self-care in Portuguese) and the first 100 for the term “self-care” in May 2019. In May 2020, one year after the first sampling and six months after the world had registered the first infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), we conducted a new search using the terms “COVID-19,” “autocuidado,” and “self-care” in the same search tools. Content suggested by the search engine that was either unavailable, duplicated, or from sources other than scientific resources (books, abstracts, or essays) were excluded from the sample. In the first stage, the data were categorized according to the following criteria: scope (Brazilian or international), field (philosophy, anthropology, sociology, psychology, clinical, education, and nursing), method (practical or theoretical), action (prevention/prophylaxis), intervention (professional orientation or health education), target population (child, expectant mother, adolescent, elderly, woman), application (specific or general health condition), expectation (empowerment, quality of life, longevity, operational for the health system), transposition of self-care as an ethical application (collective and environmental), and bioethical reference.
Our intention in the second stage was to verify the terminological application of self-care in the face of the new reality set in place by the COVID-19 pandemic, based on the following categories: origin, target population, theme, application, and transposition of self-care as an ethical application, and bioethical reference. As research variables, we compared studies undertaken in Brazil with that in other countries, while the parameters were the application of self-care, its ethical transposition to global health, and its association with the bioethical perspective.
Non-scientific communities’ conception
We also performed an integrative review of popular notions of self-care through site maps and social networks available in the Portuguese language and within the local scope so as to identify the content currently available to the population seeking information on self-care. In May 2019, upon applying the term “autocuidado,” we categorized the first 100 pages each suggested by the Google search engine, the Instagram search engine, and the Facebook search engine, and the first 100 videos recommended by YouTube. These platforms were chosen due to their popularity in Brazil and because they contain different audiences and languages. We excluded repeated suggestions or suggestions outside the context of the study from the sample. Then, we categorized the retrieved data based on the following: post date, engagement (views, likes, dislikes, and shares), public, aspect addressed (beauty, nutrition, or relationships), definition (self-responsibility, self-awareness, or maintenance), orientation, and comments.
To assess the Internet users’ position and interaction with news and videos, we recovered the 10 most recent comments for each post and categorized them according to the methodology of Fischer et al. (2018): gender, content (praise, testimony, encouragement, criticism, irony, question), and emotion (gratitude, sadness, joy, hope, love, health).
One year after this sampling, in May 2020, we identified and included 30 samples from each of these platforms to verify whether the pandemic had changed the approaches to self-care.
Data analysis was conducted using the distribution of the absolute values ??compared within each category and between variables using the chi-square test, with a 95% confidence interval.
In compliance with ethical principles, the study was conducted in accordance with the Declaration of Helsinki and Brazil’s National Health Council (CNS) Resolutions 466/12 and 510/2016 with respect to the Internet users’ integrity, anonymity, and data processing, analysis, and preservation. The project was approved by CEP/PUCPR (n. 3.855.092– CAAE: 25948719.1.0000.0020).
Results
Academic perspective
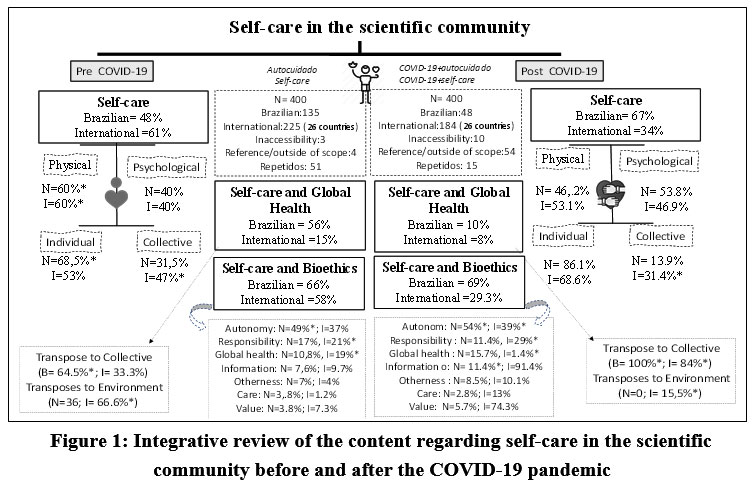
The 360 ??articles retrieved on the topic of self-care published before the COVID-19 pandemic originated from research in Brazil (37.5%) and 26 other countries: USA (27%), UK (5.5%), Colombia (4.4%), Canada (3.3%), Spain (3%), Australia (3%), China (2.5%), Mexico (2%), Sweden (1.9%), Portugal (1.5%), Chile (1.1%), India (1.1%), Italy (0.8%), Cuba (0.5%), Greece (0.5%), Lebanon (0.5%), Thailand (0.5%), Turkey (0.5%), Ireland (0.5%), Ethiopia (0.2%), Germany (0.2%), Korea (0.2%), Finland (0.2%), Netherlands (0.2%), Israel (0.2%), and Pakistan (0.2%). The 232 articles published after the pandemic originated from research in Brazil (20.6%) and 23 other countries: USA (18.5%), UK (9.9%), China (9%), Colombia (7%), Spain (5.6%), Chile (4.5%), Singapore (4%), Italy (3.5%), India (3.5%), Mexico (3%), Canada (2%), Australia (1.3%), France (0.8%), Switzerland (0.9%), Argentina (0.9%), Korea (0.4%), Netherlands (0.4%), South Africa (0.4%), Germany (0.4%), Pakistan (0.4%), Jordan (0.4%), Iran (0.4%), Puerto Rico (0.4%), and the UN (1.8%). At both times, we detected differences between Brazilian and international publications, where self-care was discussed more in the international than in the Brazilian context before the pandemic. In both scenarios, self-care was directed more toward physical and individual approaches, but after the pandemic, we observed an increase in psychological and collective approaches. This shift to the collective unit was more characteristic of Brazilian publications, whereas international publications tended to address its shift to the environment. The confluence of self-care and bioethics occurred indirectly, characterizing the Brazilian scenario by its approach to autonomy, and the international scenario by an approach to responsibility and global health (Figure 1).
.jpg) | Figure 1: Integrative review of the content regarding self-care in the scientific community before and after the COVID-19 pandemic.
|
Our analysis of the application of self-care in the scientific context before the pandemic demonstrated a tapestry of publications resulting predominantly from empirical research in the nursing field. These publications addressed the preventive nature of self-care and aimed to develop practice-based health interventions through health education to improve the quality of life of patients with specific health conditions (Table 1). Brazilian publications differed from international ones in that they focused on using the patient as a means for education and to develop the means to diagnose, empower, and provide orientation for specific groups, such as women, children, and people with kidney, circulation, or diabetic issues (Table 1). The set of scientific content we obtained after the onset of the pandemic evidenced differences. Reports and analyses in clinical research and containment measures were predominant abroad, while the main focus in Brazil was on orientation involving mainly vulnerable groups, specific professions, and collective health (Table 2).
Table 1: Characterization of scientific content published before the COVID-19 pandemic, based on area of ??knowledge, approach, topic, objective, and application.
| I | B |
|
| I | B | |
Area | Nursing | 63*a | 68*a | Application | Specific health condition | 75.0*a | 80.2*a |
Education | 4a | 13.5b | General | 25.0a | 19.8a | ||
Clinical | 17a | 13.5a |
|
|
| ||
Psychology | 11.8a | 1.3b | Patients | 85.6*a | 43.9*b | ||
Social sciences | 4a | 3.4a | Elderly | 9.8a | 21.1b | ||
|
|
|
| Women | 3.8a | 19.3b | |
Approach | Practical | 76*a | 68*a | Children and adolescents | 0.8a | 15.8b | |
Theoretical | 32a | 24b |
|
|
| ||
|
|
| Healthcare professional | 21.1a | 24.4*a | ||
Prophylaxis | 65.8*a | 57*a | Cardiac | 18.6*a | 7.7b | ||
Preventive | 35.3a | 43b | Diabetic | 18.0*a | 29.5*b | ||
|
|
| Psychiatric | 11.2a | 1.3b | ||
Health education | 57*a | 52*a | Chronic/postoperative | 11.8a | 2.6b | ||
Professional orientation | 43.2a | 48.3a | Respiratory | 2.5a | 0.0a | ||
|
|
|
| Oncologic | 2.5a | 1.3a | |
Topic | Health practice | 48.7*a | 20.5*b | Renal | 3.1a | 14.1b | |
Self-care deficit | 27.4*a | 18.3*b | Society | 0.6a | 0.0a | ||
Agent | 14.3a | 21.3*b | Circulation | 3.1a | 10.3b | ||
Education | 1.3a | - | Palliative | 0.6a | - | ||
Mental health | 5.2a | 2.2a |
|
|
|
| |
Terminologies | 2.1a | 0.8a |
|
|
|
| |
Technological impacts | 0.8a | 0.4a |
|
|
|
| |
|
|
|
|
|
|
|
|
Objective | Quality of life | 34.9*a | 26.3*b |
|
|
|
|
Longevity | 11.2a | 7.6b |
|
|
|
| |
Care | 13.6a | 12.2a |
|
|
|
| |
Diagnosis | 12.1a | 16.6b |
|
|
|
| |
Empowerment | 10.3a | 15.9b |
|
|
|
| |
Orientation | 9.6a | 19.9b |
|
|
|
| |
Operational | 8.3a | 1.4b |
|
|
|
| |
Note. Absolute values were compared within each category, and Brazilian (B) and international (I) articles were compared using the chi-square test. Significant values (P<0.05) are denoted with an asterisk (*), and significantly different means are denoted with different letters.
Table 2: Characterization of scientific content published after the COVID-19 pandemic, based on approach and procedures
|
| I | B |
|
| I | B |
Approach | Clinical | 34.9*a | 4.4b | Procedures | Report | 23.1*a | 4.3b |
Mental health | 16.6*a | 26.7*a | Orientation | 13.9 | 42.6*b | ||
Vulnerable groups (hospitalized children, individuals with autism, children, elderly, women, expectant mothers, individuals on palliative care) | 10.9a | 22.2*b | Reflection | 14.8a | 21.3a | ||
Containment measures (education) | 13.1a | 0.0b | Review | 12a | 17.0a | ||
Operational planning | 6.1a | 11.1a | Opinion | 7.4a | 6.4a | ||
Professions (odontology, geography, OT) | 3.9a | 13.3b | Analysis | 22.7a | 0.0b | ||
Medical team | 7.9a | 6.7a | Questionnaire | 6a | 4.3b | ||
Behavior (representation, domestic violence, rights) | 4.4a | 4.4a | Legislation | 0.0a | 4.3a | ||
Diagnosis of situation | 1.3a | 4.4a |
|
|
|
| |
Collective health | 0.9a | 6.7b |
|
|
|
|
Note. Absolute values were compared within each category, and Brazilian (B) and international (I) articles were compared using the chi-square test. Significant values (P<0.05) are denoted with an asterisk (*), and significantly different means are denoted with different letters.
Non-scientific perspective
Application of the term self-care on social networks presented a stronger relationship with physical and mental well-being, and we did not detect differences after the pandemic, especially in Instagram posts, wherein its association with self-awareness and self-love for women’s well-being was predominant. On the other hand, Facebook already had numerous groups focusing on COVID-19 and demonstrated an increase in the association between self-care and its approach toward providing support and care for the other and a decrease in community bias. On YouTube, posts were directed toward physical and mental well-being and showed an increase in the direction of maintenance and health after the pandemic (Figure 2). Although the content posted on websites and blogs still associated self-care with individual behaviors, whether physical or mental, the posts were impacted after the pandemic in that the focus on behavior and health turned to the news. The word cloud associated with the term shows a wide range of interrelations of individual attitudes, but with connections to relationships and nature, which were exceeded by leisure and hygiene after the pandemic (Figure 4).
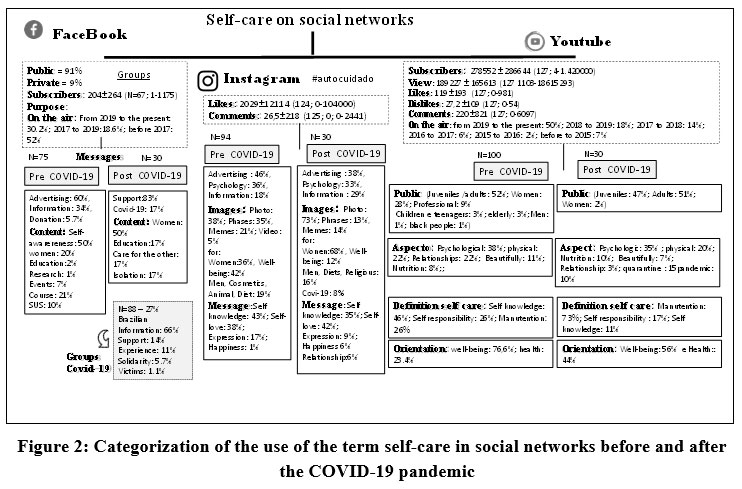 | Figure 2: Categorization of the use of the term self-care in social networks before and after the COVID-19 pandemic
|
 | Figure 3: Categorization of the use of the term self-care in non-scientific communities media.
|
The netizens who were inclined to engage with the YouTube posts were predominantly women who were satisfied with the content and demonstrated gratitude and praise. Self-care was related with mental and individual aspects. Nevertheless, the pandemic led to an increase in its association to the population as a collective whole, which is evident in the analysis of the word cloud related to the term, wherein self-awareness made space for connection and empathy, as evidenced by the offer of tips on how to face social isolation (Figure 4, Chart 1).
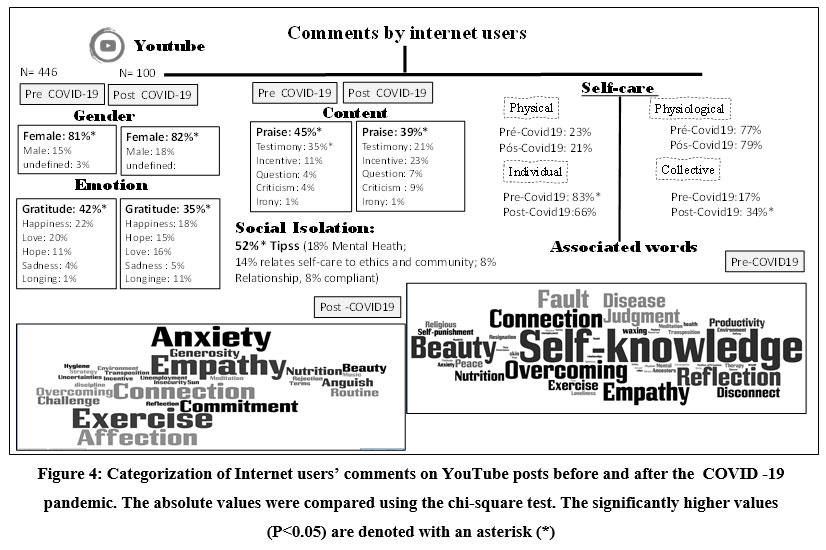 | Figure 4: Categorization of Internet users’ comments on YouTube posts before and after the COVID -19 pandemic. The absolute values were compared using the chi-square test. The significantly higher values (P<0.05) are denoted with an asterisk (*)
|
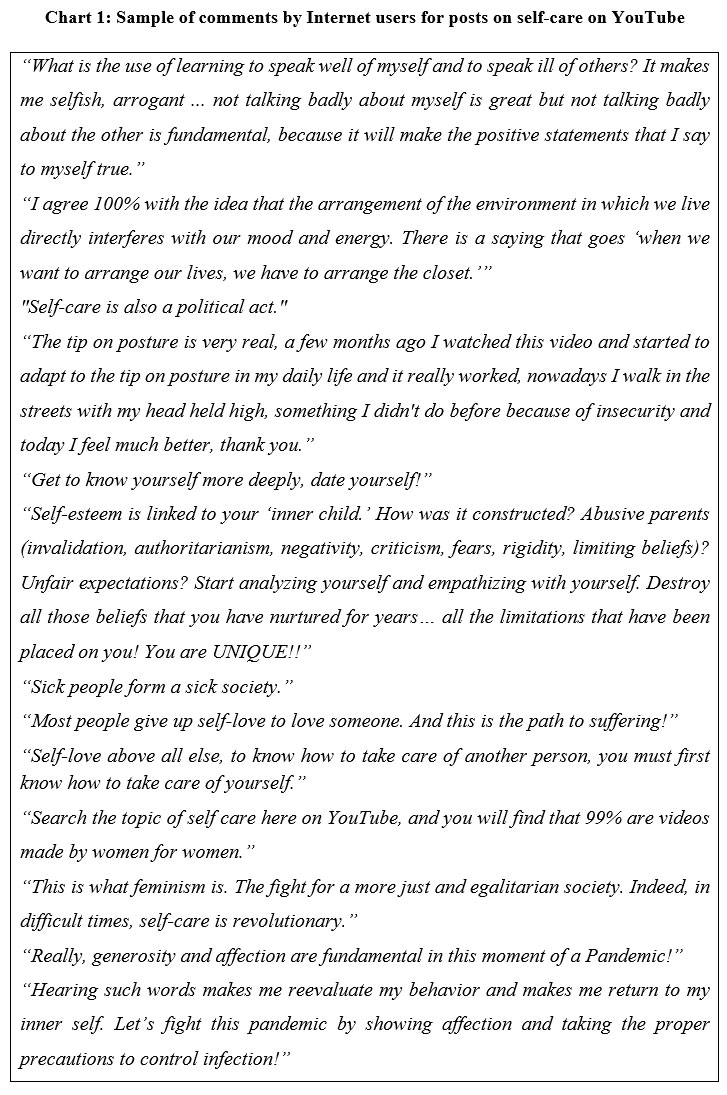 | Chart 1: Sample of comments by Internet users for posts on self-care on YouTube.
|
Discussion
Based on the sample in this research, the results demonstrated dissonance between the approach to self-care in academic and non-scientific communities circles, presenting changes after the COVID-19 pandemic in terms of amplification of the term and its inclusion in debates on global health and environmental bioethics. The present study potentially contributes to scientific literature, as the interpretive pathways resulting from the analysis of the methodological approach allow for the expansion of the self-care terminology. The term self-care, which has predominantly been used in clinical contexts to educate patients on collaborating with medical teams, finds in the community and in the relationship with the environment the possibility of expanding individual benefits of maintaining good health. The realization that popular perspectives do not correspond to scientific ones demonstrates a gap that is starting to be minimized by analyzing societal behavior following the experience of the COVID-19 pandemic.6,7,8,9,12
Employment of the term self-care in the scientific context occurred mainly indirectly, associated with the field of nursing, studies related to prophylactic measures in health education and practice in the pursuit to promote quality of life for patients with a specific health condition. In general, self-care was adopted as a diagnostic measure for planning actions of care within a clinical context. Although the concept of self-care was appropriated in the field of nursing3 highlights its transversal and interdisciplinary nature as it covers different segments, such as sociology, anthropology, politics, and economics. According to Silva et al. 2, self-care is salient in nursing because the nurse is the closest and most dedicated professional to the sick individual; consequently, they are the ones who witness the patient’s suffering the most, and their assistance is fundamental. Bub et al.13 noted that self-care in the field of healthcare is widely addressed in nursing possibly because the first person to apply the concept was a nurse. Dorothea Orem created the theory of self-care and the self-care deficit nursing theory1, especially developing the concept to establish a system capable of organizing nursing practices in their specificity.
The association of self-care to health practices and education occupies a space that demands references and orientation, especially among the healthcare team, who are the ones who exercise less self-care10,14, which Tobón-Correa3 defines as a behavioral paradox, wherein the person has the information but adopts risky behavior. According to Cruz14, this conduct is often due to an exhausting routine, little time to take care of appearances and diet, and a perspective of symptom-control through self-medication15. Silva et al. 2 state that aside from the professionals’ need to develop and improve knowledge regarding care for others, they will be able to provide care for the patient based on a good understanding of self-care, thus promoting the development of the care provider and the person cared for. Baggio15 maintains that professionals who take care of themselves by providing care for the other have better tools for coping with conflicts, and the construction of self-care is perceived from the meanings attributed to the practice of caring for the other. This perspective, which had already been observed, intensified after the onset of the COVID-19 pandemic.16 Gallasch, Cunha, Souza & Silva-Junior17 reported failures in personal protective equipment (PPE) use and frequent exposure to infected patients, in addition to an increased intensification of working hours and greater social complexity and hostility. As a result, the number of infected health professionals increased in several countries as they compromised their own protection.17
Patient education in self-care provides support for nursing efforts. According to Santos and Marques18, the nurse assumes the role of health information provider by focusing on the aspect of disease prevention and support to specific patient groups and uses the self-care deficit as a diagnosis, as imposed by the professional code of ethics which exalts the nursing profession in favor of the benefits for the person, family, and community. Sampaio and Guedes19 stressed that nursing is considered a supportive, facilitating profession, which implements health education and promotion strategies and redefines the condition of the conscious patient. It is also a necessary learning experience with regard to the specificities of some diseases20. However, the studies we analyzed demonstrated that there is still an inclination toward prophylactic interventions for specific diseases, which probably characterize the local community and the real need to mitigate problems that are already in place and do not provide space for preventive actions. Lima et al. 20 indicated the nurses’ insufficient knowledge about risk factors, prevention, and self-care related to many diseases and the need for constant training to optimize early detection and contain the progression and chronification of the disease. For Rocha and Santos21, Brazil still needs public policies that favor self-care education centered on the person and their responsibility along with the healthcare team.
The data from our categorization of the scientific content confirmed the hypothesis of the differences in approaches to self-care within the Brazilian and international contexts. Research in Brazil presents some peculiarities, such as greater involvement with ??education and the clinical area, preventive measures, the use of the self-care deficit as a diagnostic parameter, the training of agents and their empowerment through orientation with a focus on vulnerable groups. International studies distinguished themselves by presenting more theoretical research in the area of ??psychology, health practices and quality of life in cardiac, psychiatric, and chronic patients. Langdon et al.22 observed that Brazil is peculiar in terms of perspectives and social and political aspects that differ from healthcare in the North Atlantic. Consequently, cultural and social forces and representations of the body and diseases are relationally-constructed aspects. The Brazilian Unified Health System (SUS) was implemented along with the constitution in 1988, thus constituting the largest policy of social inclusion in the country, based on the human and constitutional right to health in its aim toward ensuring universal health. Even with great challenges related to the system’s fragmentation; low public investments; and lag time due to demographic, nutritional, and epidemiological transitions, it stands out for its Primary Health Care (PHC). Its PHC has garnered better results in reducing mortality and costs and accessing preventive services. Pacheco and Antunes23 stressed that PHC, through self-care education in health, promotes the quality of life and empowerment of individuals and social groups, thereby providing them with the strength to face challenges aligned with the needs of the local community. These authors have related self-care to identification with beliefs and knowledge, which are favored by popular communities conversation circles, whose sensitized communities, with access to information, are motivated to transpose their paradigms. Even Nascimento and Oliveira24 emphasized the implementation of integrative and complementary and group practices in PHC as a means of favoring complex approaches to the health-disease process, thereby allowing the democratization of services hitherto restricted to the private sector. As for the challenge of harmonizing with the users’ needs, the author proposed the expansion of the practices offered (relaxation; meditation; yoga; tai chi; and the groups of care providers, women, the elderly, embroiderers, walking, storytellers, art therapy, community therapy, theatre of the oppressed) to other areas that are integrated with cultural realities (homeopathy, acupuncture, traditional Chinese medicine, thermalism (hydrotherapy), anthroposophical meditation, phytotherapy, reiki, and lian gong). Nascimento and Oliveira24 reinforced the importance of a space for dialogue, creativity, articulation of knowledge, and practices of solidarity as promoters of demedicalization, demercantilization, and enrichment. This approach undoubtedly promotes the strength of SUS as a political resistance and generator of new knowledge and practices that redefine self-care.
The pandemic influenced the application of self-care with the intensification of clinical analyses and reports and containment measures in international research and with orientation and questionnaires for vulnerable groups and professionals and public health in Brazilian research. Due to the timing of the onset of the pandemic in the country, the profile of Brazilian research probably reflects a two-month delay when compared to countries in the North Atlantic that already have enough data to report and analyze, while in Brazil the demand is for orientation. In both the scenarios, there was a more pronounced focus on mental health in the research, which demonstrates that the pandemic’s impact on the population moved beyond physical damage, which was oftentimes fatal. For Braus and Morton25, the pandemic brought forth two enemies: the unknown virus and mental health challenges. Instructions for flattening the curve and social isolation measures triggered countless consequences in different manners, affecting everyone from the lonely single person to the unemployed family man to the new work and study routine at home to the professionals in essential services or on the front line who must deal with unmitigated stress, emotions, and trauma. Spoorthy, Pratapa and Mahant26 underscored that pandemic situations can cause serious illnesses and variable psychological effects, in addition to worsening prior conditions and the emergence of new ones. The author suggested that authorities should consider the creation of multidisciplinary mental health groups at the regional and national levels and promote support to patients and medical teams, using technology as a means. According to Medeiros et al.27, becoming aware of the importance of physical, mental, and social self-care constitutes an essential challenge for global health institutions to create support for the population’s health.
The onset of the pandemic changed the approach to self-care in Brazilian and international research. Brazilian publications exceeded international publications in furthering the concept of self-care, and its association with physical behaviors has been transferred to mental ones. The connection to collective behaviors was more evident in international publications. However, inserting relationship aspects as a requirement for self-care, as suggested by Santos et al.28 for quality aging, does not necessarily explain the transposition to the positive impact of self-care in the community, as evidenced in national surveys. Holguín and Sandoval29 highlighted that promoting self-care is a form of humanization, since it enables the conversion of the individual into a subject and enables investment in life within the context of society. However, it is noteworthy that the transposition of self-care as environmental improvement was not too evident in Brazilian publications and was more prominent in international ones. Tobón-Correa3 proposed that self-care is conditioned by internal (education, will power, values, experience, motivations, and habits) and external factors, such as culture, gender, technoscience, and ecological factors, which is based on the premise that everything that happens on the planet is related to self-care. Tarazona-Modes30 warned that the relationships established with nature and with animals involve an individual, collective, and governance responsibility, the negligence of which can result in situations such as those experienced with COVID-19. However, the author indicated that so many other pandemics could arise due to the consumption of animals in other cultures, the domestication of wild animals, the destruction of ecosystems, the exploitation of natural resources, and global warming. For Tarazona-Modes30 although the world is mobilizing to contain the pandemic, it is necessary to rethink the causes and our relations with nature, animals, and people as components of self-care.
The confluence of self-care with the bioethical perspective was also more evident in Brazilian studies, both before and after the pandemic. The characteristics of Latin American bioethics probably provide more of this dialogue than the North American bioethics. For Hossne31, even after its 40 years of existence, the North Atlantic countries still practice bioethics based on principlism, promulgating the principles of autonomy, beneficence, nonmaleficence, and justice, which has, consequently, a more individualistic and analytical character, involving the search for quality of life through the application of the principles of responsibility and global health, as confirmed in this study. In contrast, Latin American community bioethics corresponds to the data with a greater number of justifications for self-care interventions in search of empowerment. According to Feitosa and Nascimento32, bioethics in Brazil prevails in the social environment, with emphasis on intervention bioethics, a branch of social bioethics idealized by Garrafa33, which has been linked to social movements in defense of public health since the origin of the health reform movement of the 1980s.
The sudden global change in the face of the COVID-19 pandemic brought about a mobilization of the scientific community that started to analyze the issue from different perspectives. Nonetheless, although the most effective measure to contain the infection is social distancing, which was adopted worldwide, it did not meet the expectations of this study in that there would be a change in the approach to self-care.6 Given that the pandemic introduces broader connotations into the individual context, as preventive measures do not benefit only the agent but also the collective unit, including those who are close or dear, vulnerable, unknown, or even the entire healthcare system. The meeting of bioethics with pandemics has a space for discussion in global bioethics.7 For 10 years, Goldim34 has questioned the ethical, legal, and social aspects related to the (H1N1) influenza pandemic, which is applicable in the current situation. For the bioethicist, bioethics can use four models to draw inferences from this issue: the virtues, ethical principles, human rights, and otherness; however, fear and anxiety will only be supplanted with clarifications through clear, truthful, and accessible information. Discussing bioethics and the pandemic must transpose critical decisions on the allocation of resources at the time of the pandemic to minimize mortality and morbidity, as recommended by Bergallo et al.35, but consider preventive measures. For Machado, Gonçalves and Arcanjo36, the pandemic materializes the consequences of a capitalist logic that is unsustainable for public health; although the contagion is democratic, access to the means of survival as an individual and as nations is not.
The perspective of environmental bioethics also assigns the use of values ??so that decisions are made on collective rather than personal interests. Santos et al.28 and Rosaneli, Brotto, Pieri & Fischer12 emphasized that age or illness does hold that much influence on people's decisions related to their self-care as much as values ??and experiences; consequently, references that emerge from the social, cultural, or personal structure shape self-care through the experience of falling ill. In this context, the importance of having access to clear, truthful information that adds meaning to actions of self-care is evidenced once again, especially in borderline situations.
Social networks and non-scientific communities’ websites presented a different view of self-care compared to the scientific community’s approach, focusing on individual, physical, and mental actions centered on self-awareness, self-esteem, empowerment, and well-being for a predominantly female audience. The content presented guidelines on female empowerment, understood as a resource for reducing inequalities and for individual and collective decision-making, aimed mainly toward decreasing the unequal distribution of power. Marinho and Gonçalves37 claim that groups have been using diversified strategies to promote personal and social changes in the engagement of women hitherto represented as sensitive, emotional, and passive. On the other hand, Gomes et al.38 related that the man’s representation as the strong, manly family provider can also be a factor of vulnerability, since he considers self-care to be futile and postpones seeking medical help in case of illness, which results in more serious, often fatal, problems. Qiu et al.39 pointed out that in China there were more men who were contaminated by COVID-19 than women. Lima et al.20 reported that even though men were more prone to the virus, they were the most negligent and did not voluntarily quarantine.
Self-awareness was the biggest factor related to self-care on social networks and non-scientific communities digital content platforms. For Brandenburg and Weber40, self-awareness is a tool that can be used to improve the quality of life and allow. Therefore, more self-awareness means a more realistic, objective perception, which means better adaptation to life’s circumstances, consequently making self-care feasible. Meditation, writing, contact with nature, and relationships were words that stood out in the guidelines posted on non-scientific communities media. Votto and Carvalho41 evaluated 50 meditation practitioners and evidenced the positive effects of self-awareness and self-acceptance on individuals’ physical and mental well-being, as they promote the management of daily stressors, relaxation, mental freedom, and autonomy in identifying realistic interpretations42. Tobón-Correa3 related self-care to diet, hygiene, stress control, close relationships, physical exercise, medication control, safe behaviors, and leisure, but stressed that the degree of importance changes depending on the circumstances.
Beauty-oriented physical self-care was appropriated by social networks. Although at first glance it can be seen as more futile than health-related self-care discussed in the scientific community, it establishes a relevant relationship with the collective unit. Prasad and Mehendale9 conducted an analysis of 100 self-care related posts on social media platforms, and despite variations in approach, they arrived at the conclusion that the virtual sphere harbors significant potential for educational purposes. For Baggio15, esthetics materializes self-care and reminds one that they must take care of the other in the same way. Thus, it projects the individual action and feeling of beautification by favoring togetherness, since life acquires value in the same measure as one favors the desire to be with another person. Nevertheless, this perspective opens space for appropriation by marketing, as observed on the social networks Instagram and Facebook. Castiel43 underscored the compulsion felt by contemporary society to be able and willing to face a dysfunctional reality; it stimulates the consumption of products, services, and ideas. This solidifies the “ethics of manipulation” referred to by Bergallo et al. 35, whose information is conducted by dominant groups for submissive, impressionable citizens with a compromised capacity for reflection and autonomy.
Non-scientific communities approaches were also impacted by the pandemic. Although the topic did not occupy all the space as expected, issues such as education, how to deal with the quarantine and the pandemic, care for others, and physical and mental health were introduced. Society suddenly found itself in a unique situation in which it had to deal with unprecedented problems without prior experience or tools to face such critical issues with long-term individual and social repercussions. Wallace et al.44 addressed the issue of mourning affecting patients, families, institutions, and governments, losses that alter life, including loss of health, freedom, and economic security. According to the authors, there is a merging of typical and new processes (e.g., distancing, isolation, uncertainty, guilt, impossibility of mourning or burying the dead). Weaver45 highlighted the importance of talking to children and informing them of historical contexts wherein other diseases impacted societies, how cures were discovered, how people came together to promote hope. They stressed that it is important to place them in the generational lineage by exploring family photos and stories of the elderly and connecting them to a larger narrative. In both cases, the authors suggested using the principles of palliative care to establish welcoming communication based on the principles of honesty, trust, self-compassion, security, sensitivity, connection, preparation, community building, death as part of life cycles, and legacy.
Although it has not demonstrated a direct appropriation of self-care as an ethical, political, community, or humanitarian conduct, the content addressed in non-scientific communities media after the pandemic began to relate words associated with the collective unit at a time when isolation led one to question the importance of relationships. Braus and Morton25 suggested art therapy as an efficient, accessible, and low-cost way to promote self-care and as a healthy outlet for emotions intensified by the pandemic. They proposed that through mindfulness and self-expression, it is possible to connect fear and anxiety with positive sensory expressions that allow one to cope with and control emotions. Braus and Morton25 described in the US a reality that was also experienced in Brazil, wherein people are creating masks, trying recipes, creating fun videos, and sharing music with the neighbors.
Internet users' comments allowed access to the representation of self-care, for example, a female user who expressed satisfaction with the content consumed, the implications of which still prevail. This is a different result from that obtained by Fischer et al.46 when they assessed social participation after news about the water crisis came to light. At the time, the predominantly male comments demonstrated a highly aggressive tone and critical and political content, which led the authors to interpret them as a failure in communication related to the demands of nature, population, and political and economic interests, which constitute the limits to the Internet’s effectiveness in the process of ethical awareness. This is probably owing to the fact that the interactions of Internet users and content creators recognize self-care as a female-dominant activity. Fischer et al.47 questioned whether the Internet could constitute a space for the development of an ethical conception since the challenges of bringing the virtual citizen’s participation to concrete spaces of social control are numerous. However, the authors consider that the difficulties identified should not prevent the proposition of communication strategies and participation from different sectors of the collective sphere in the technical, political, ethical, and social debate. Therefore, they consider that the digital space has the potential to be the place for greater qualification of information and social formation and ethical awareness.
The public that accesses personal channels is interested and satisfied with consuming contents where they find orientation for their own self-understanding and self-care. This demand, although recent, already has a great variety of information considering their predominance in recent years, the large number of subscribers, content sharing, and interaction, leading to the possibility of risk that information based on personal perceptions and mainly devoid of technical bias is likely to be influenced by marketing. Barbosa48 attested that mainly the young audience has preferred searching for information on digital media, since channels allow for the constitution of groups based on common and specific interests, thereby generating the sense (or desire) of belonging49, identifying the other as an interpersonal relationship48. Minerbo50 added that the pleasure of this relationship lies in the intimacy of sharing and spreading the imperfections of being and in identification with the YouTubers’ weaknesses, fears, failures, and insecurities. This individual, according to Barbosa48, experiences the company of another equal in this virtual intimacy. Conversely, given that anyone can generate content and claim that it is true, there is a concern that Internet users do not have the tools, among the endless options, to filter those that can actually contribute to their self-care. Drawing a parallel to Bauman51, in the existence of a culture that does not value quality, the market of emotions with (dis)satisfactions is always constant, aspiring to become the news, the search for a consumer culture favors products ready for immediate use, even if their results are momentary and do not guarantee their veracity. For Bauman51, the individual with their freedom of choice and consumption represents a vector of wear for the citizen who must focus their well-being on the needs of the collective unit. Farias and Monteiro52 consider that users can put aside their intellectual growth to give way to the satisfaction of their egos with information created and conveyed for this purpose. This pattern becomes more worrisome when the content transmitted is related to aspects focused on public health, the distorted interpretations of which could have serious consequences for both the individual and the community. Castiel43, Fischer et al.47, and Palodeto and Fischer4 stressed that despite the Internet’s libertarian and democratizing perspective, there are cultural prerequisites to its access, which make the user vulnerable. According to Moretti et al.53, there has been a mobilization of institutions to standardize, regulate, certify, and monitor health information made available on the Internet. Castiel43 discussed the domains of e-health as the mediation between information, health professionals, and clients in promoting patient/consumer autonomy in PHC to reduce decisive conflicts. Thus, it would be possible to monitor the quality of information and educate the consumer to certify the information’s quality. The current reality promotes the immediate public disclosure of scientific findings, so there is no way to disregard this new patient, who today represents about 75% of people with Internet access. Castiel43 argues that there is an urgent need to stop the generation of these proto-patients without doctors in consumers who attribute citizen status to the well-informed consumer.
The risks and the fight against fake news have intensified at this moment of the pandemic. After the onset of COVID-19, when investigating the approach to the topic on YouTube (just over a month since the quarantine in Brazil), to demonstrate that the topic of self-care related to the pandemic is growing at an accelerated pace, it is worth noting that more than 300 videos were published in one month with content related to care for physical and mental health, hygiene, and other preventive measures. According to Cruz et al.14, this is due to the new, unexpected moment of this crisis and emergency, which carries social, economic, and physical and mental health impacts on populations, especially the most vulnerable. The current reality of confinement and isolation conditioned by the pandemic demands a search for security, support, and orientation. This unexpected fact with global consequences clearly elucidates the liquidity of information and interests and how to direct the tools toward specific needs. If until a month ago the search was for guidance on how to like oneself more, now the question is how to take care of oneself and others.
Final considerations
Analysis of the application of the term self-care, allowed by the sample in this study, revealed a divergence between scientific and non-scientific communities approaches and supporting the proposal to expand the scope of the term in order to include aspects related to global health. As attested by Palodeto and Fischer4 for self-care to be introduced in the terminology "conscious use of medicines", the terminology’s limitation must be considered as potentially restricting conceptions and causing delays in interventions. Non-scientific communities content and participation from Internet users show that there is a demand for orientation on exercising self-care with a mental and community bias that, due to gaps in the scientific environment, becomes appropriated by the population that generates and propagates content that is often based on personal perceptions. The new knowledge added by this study shows the legitimacy on the appropriation of the topic at the confluence of environmental bioethics and global health, mainly because it limits the citizen to access suitable and complete information. Within the context of the conscious use of medication, the differences between the scientific and popular communities, according to Palodeto and Fischer4, can impact citizens who do not understand themselves as agents in the transposition of self-care to global health issues. Consequently, the question’s introduction into bioethical debates calls for the inclusion of body/mind/spirit, individual/collective/environmental, and local/global interconnections in self-care terminology, thereby encompassing the social, individual, environmental, and communicative dimensions. The environmental bioethics perspective stresses the importance of values ??in the decisions of moral agents and the potential to cause vulnerabilities if they aim to supplant only personal interests. Strengthening of respect for human rights is commanded by an understanding that physical, mental, and individual health will only facilitate improvements in quality of life if the community around the individual is also healthy. This perspective has been clearly evidenced with the COVID-19 pandemic; although it is not unprecedented, it is the first major global event experienced by the current generation. In this context, self-care not only protects what is cared for, but taking care of oneself also prevents others from getting sick and becoming a risk. The pandemic personifies life's unpredictability, bringing about the realization that many references for security no longer have the same value, such as economic power, which does not guarantee access to medical care in a collapsed system and does not allow exploration of the possibilities of a world with closed borders.
Decision-making for self-care requires a critical, autonomous, and proactive conscience that one is mainly responsible for the results and consequences of their own actions. Therefore, self-care and health must be valued even in the absence of disease that is prevented in a physical, emotional, social, and spiritual environment that sustains quality of life for oneself and others. Thus, it is necessary to reframe the health-disease paradigm through educational policies that prioritize autonomy. Obviously, a citizen with limited access to qualified information will be vulnerable to deep-rooted cultural beliefs, the influence of marketing, and immediate individualistic standards. For Palodeto and Fischer5 terminological products enable communication without noise among the public, private, and academic spheres. This is especially important in collective health interventions to simplify communication by relating concepts and values ??and supporting supervision and assessment in the health-disease representation process.
Self-care as a unique individual practice that is acquired and varies according to the environment must consider the bio-psycho-social being and their balance for global health. Self-care is defined as a viability of the activities promoted by the personal care required daily to regulate one’s own functioning and development. The scientific contribution of this research supports the appropriation of the dialogical, deliberative, and regulatory nature of bioethics underlies the importance of the educational process in the formation of a citizen who understands self-care as a biological and ethical principle and is capable of recognizing their responsibility to their own existence in their cultural, social, and environmental relations. Therefore, the findings of this research, and the resulting interpretative trails, support the proposal of the self-care as an ethical principle understands that taking care of oneself is being whole for the experiences that life can provide; it is being better for the other, for nature, and for future generations who may enjoy the existence of a being with integral health and does not deliberate for the other to bear the consequences of their choices.
Acknowledgments
The Editage that translated the article.
Conflict of Interest
The author(s) declares no conflict of interest.
Funding Sources
There are no funding sources.
References
- Orem, D. (2001). Concepts of pratice. Mosby; 6 ed.
- Silva, I. J., Oliveira, M. F. V., Silva, S. E. D., Polaro, S. H. I., Radunz, V., & Santos, E. K. A. (2008). Cuidado, autocuidado e cuidado de si: uma compreensão paradigmática para o cuidado de enfermagem. Revista da Escola de Enfermagem da USP, 43, 697–703.
CrossRef - Tobón-Correa, O. (2003). El autocuidado una habilidad para vivir. Hacia promoc. salud, 37-49.
- Palodeto, M.F..T, & Fischer, M. L. (2019). Apropriação da terminologia ‘uso consciente de medicamentos’ visando à promoção da saúde global. Revista Eletrônica de Comunicação Informação e Inovação em Saúde. 13(1),191-207. https://doi.org/10.29397/reciis.v13i1.1438
CrossRef - Palodeto, M.F.T & Fischer, M. L. (2018). A representação da medicamentação sob a perspectiva da Bioética. Saúde & Sociedade. 27, 252-267. https://doi.org/10.1590/S0104-12902018170831
CrossRef - Fischer, M. L., Cunha, T. R. D., & Burda, T. A. M. (2021). Perspectivas de brasileiros durante a pandemia da Covid-19: uma análise sobre autocuidado e bioética ambiental. Saúde em Debate, 45, 733-747. DOI: 10.17765/2176-9206.2022v15n1.e9948
CrossRef - Fischer, M. L., Burda, T. A. M., & Rosaneli, C. F. (2022). O autocuidado para saúde global: um compromisso ético com a coletividade. Holos, 38(4), e12844. DOI: 10.15628/holos.2022.12844.
- Rodríguez-Cánovas, B., Rogala, A., & Rincón, AG (2022). Comportamiento de autocuidado y de búsqueda de información en internet sobre la COVID-19. International Visual Culture Review, 9, 1-11. https://doi.org/10.37467/revvisual.v9.3639
CrossRef - Prased, A., & Mehendale, S. (2023). Self-care: A thematic study of self-care posts amidst COVID-19 on Instagram. In AIP Conference Proceedings (Vol. 2523, No. 1, p. 020097). AIP Publishing LLC. https://doi.org/10.1063/5.0110011
CrossRef - Oliveira, M. D. & Fischer, M. L. (2022). Autocuidado na educação física na perspectiva da bioética: uma revisão integrativa. Revista Inclusões 9 (Especial):71-97. https://doi.org/10.58210/fprc3392.
CrossRef - Mendes, K. D. S., Silveira, R. C. D. C. P., & Galvão, C. M. (2008). Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto & contexto enfermagem, 17(4), 758-764.
CrossRef - Rosaneli, C. F., Brotto, A. M., Pieri, L. G., & Fischer, M. L. (2021). O legado ético no enfrentamento da pandemia covid-19: a sinergia entre a perspectiva global e a identidade regional. Holos, 4, 1-19. https://doi.org/10.15628/holos.2021.11414
- Bub, M. B. C., Medrano, C., Silva, C. D. D., Wink, S., Liss, P. E., & Santos, E. K. A. D. (2006). A noção de cuidado de si mesmo e o conceito de autocuidado na enfermagem. Texto & Contexto-Enfermagem, 15, 152-157. https://doi.org/10.1590/S0104-07072006000500018
CrossRef - Cruz, R. M., Borges-Andrade, J. E., Moscon, D. C. B., Micheletto, M. R. D., Esteves, G. G. L., Delben, P. B., ... & Carlotto, P. A. C. (2020). COVID-19: emergência e impactos na saúde e no trabalho. Revista Psicologia Organizações e Trabalho, 20 (2), I-III. http://dx.doi.org/10.17652/rpot/2020.2.editorial
CrossRef - Baggio, M. A., & Formaggio, F. M. (2007). Profissional de enfermagem: compreendendo o autocuidado. Revista Gaúcha de Enfermagem, 28(2), 233.
- Murphy, J., Farrell, K., Kealy, M. B., & Kristiniak, S. (2023). Mindfulness as a self-care strategy for healthcare professionals to reduce stress and implicit bias. Journal of Interprofessional Education & Practice, 100598. https://doi.org/10.1016/j.xjep.2022.100598
CrossRef - Gallasch, C. H., Cunha, M. L., Souza, L. A. P., & Silva-Junior, J. S. (2020). Prevenção relacionada à exposição ocupacional do profissional de saúde no cenário de COVID-19. Revista Enfermagem UERJ, 28: 49596. ttps://doi.org/10.12957/reuerj.2020.49596
CrossRef - Santos, S. G. F. D., & Marques, I. R. (2006). Uso dos recursos de Internet na Enfermagem: uma revisão. Revista Brasileira de Enfermagem, 59(2), 212-216.
CrossRef - Sampaio, C. D. F., & Guedes, M. V. C. (2012). Processo de enfermagem como estratégia no desenvolvimento de competência para o autocuidado. Acta Paulista de Enfermagem, 25(2), 96-103.
CrossRef - Lima, W. L. D., Paula, L. B. D., Duarte, T. T. D. P., & Magro, M. C. D. S. (2020). Conhecimento dos enfermeiros da atenção primária à saúde sobre fatores de risco para Lesão Renal Aguda. Escola Anna Nery, 24(2), 1-7. http://dx.doi.org/10.1590/2177-9465-ean-2019-0280
CrossRef - Rocha, R. D. P. F., & dos Santos, I. (2009). Necessidades de autocuidado entre clientes com doença renal crônica: revisão integrativa de literatura. Revista de Pesquisa Cuidado é Fundamental, 1(2), 423-433.
- Langdon, E.J., Follér, M.L., Maluf, S.W. (2012). Um balanço da antropologia da saúde no Brasil e seus diálogos com as antropologias mundiais. Anuário Antropológico, 1, 51-89.
CrossRef - Pacheco, A. E., & Antunes, M. J. M. (2015). Revisão da literatura sobre motivação para o autocuidado na Atenção Primária em Saúde. Revista Eletrônica Gestão e Saúde, (3), 2907-2918.
CrossRef - Nascimento, M. V. N. D., & Oliveira, I. F. D. (2016). As práticas integrativas e complementares grupais e sua inserção nos serviços de saúde da atenção básica. Estudos de Psicologia, 21(3), 272-281.
CrossRef - Braus, M. & Morton, B. (2020). Art Therapy in the Time of COVID-19. Psychological Trauma: Theory, Research, Practice, & Policy. Advance online publication. http://dx.doi.org/10.1037/tra0000746
CrossRef - Spoorthy, M. S., Pratapa, S. K., & Mahant, S. (2020). Mental health problems faced by healthcare workers due to the COVID-19 pandemic–A review. Asian journal of psychiatry, 51, 102119. https://doi.org/10.1016/j.ajp.2020.102119
CrossRef - Medeiros, A.Y.B.B.V., Pereira, E.R, Andrade, R.M..CR. & Araujo F. (2020). Fases psicológicas e sentido da vida em tempos de isolamento social pela pandemia de COVID-19 uma reflexão a luz de Viktor Frankl. Research, Society & Development, 9(5), e122953331. https://doi.org/10.33448/rsd-v9i5.3331
CrossRef - Santos, I. D., Alves, A. C. D. S., Silva, A. F. L. D., Caldas, C. P., Berardinelli, L. M. M., & Santana, R. F. (2011). O grupo pesquisador construindo ações de autocuidado para o envelhecimento saudável: pesquisa sociopoética. Escola Anna Nery, 15(4), 746-754.
CrossRef - Holguín, E.C. & Sandoval, P.R.G. (2020). Resistir la Covid-19. Intersecciones en la Educación de Ciudad Juárez, México. Revista Internacional de Educación para la Justicia Social, 9(3), 7-23. https://doi.org/10.15366/riejs2020.9.3.001
CrossRef - Tarazona-Morales, A. M. (2020). Relaciones en tiempos de pandemia: COVID-19 y bienestar animal, ambiental y humano. Revista Facultad Nacional de Agronomía Medellín, 73(2), 9128-9130.
CrossRef - Hossne, W.S. (2006). Bioética – princípios ou referenciais?. O Mundo da Saúde. São Paulo: Bioetikos, 4(30), 673-676.
CrossRef - Feitosa, S. F., & Nascimento, W. F. D. (2015). A bioética de intervenção no contexto do pensamento latino-americano contemporâneo. Revista Bioética, 23(2), 277-284.
CrossRef - Garrafa, V. (2006). “Redbioética – Uma iniciativa da Unesco para a América Latina e o Caribe”: http://www.unesco.org.uy/ci/fileadmin/shs/redbioetica/revista_1/Revista1.pdf .
- Goldim, J.R. (2009). Bioética e pandemia de influenza. Revista HCPA, 29(2), 161-166.
- Bergallo, A., Salerno, R., Campodo?nico, R., Tropea, O., Baikauskas, G., Echelini, M. F., ... & Andreatta, P. (2020). Bioética y pandemia. Revista do Hospital El Cruce, 4,1-7.
- Machado, B.S.M, Gonçalves M.V.F & Arcanjo M.F.G. (2020) Neoliberalismo em tempos de coronavírus ou coronavírus em tempos de neoliberalismo?. Espaço e Economia Revista brasileira de geografia econômica, 18 (IX), 18 1-8 https://doi.org/10.4000/espacoeconomia.12379
CrossRef - Marinho, P. A. S, & Gonçalves, H. S. (2016). Práticas de empoderamento feminino na América Latina. Revista de estudios sociales, (56), 80-90.
CrossRef - Gomes, R., Nascimento, E. F. D., & Araújo, F. C. D. (2007). Por que os homens buscam menos os serviços de saúde do que as mulheres? As explicações de homens com baixa escolaridade e homens com ensino superior. Cadernos de Saúde Pública, 23, 565-574.
CrossRef - Qiu, J., Shen, B., Zhao, M., Wang, Z., Xie, B., & Xu, Y. (2020). A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Archives of general psychiatry,33(2), e100213. https://doi.org/10.1136 / gpsych-2020-100213
CrossRef - Brandenburg, O.J., & Weber, L.N.D. (2005). Autoconhecimento e liberdade no behaviorismo radical. Psico-USF 10(1), 87-92.
CrossRef - Votto, G. G., & de Carvalho, H. W. (2019). Bem-estar psicológico e meditação: um estudo associativo. Estudos Interdisciplinares em Psicologia, 10(3), 60-75. https://doi.org/10.5433/2236-6407.2019v10n3p60
CrossRef - Ricard, M. (2007). Felicidade: A prática do bem-estar. São Paulo, SP: Palas Athena.
- Castiel, L. D., & Vasconcellos-Silva, P. R. (2002). Internet e o autocuidado em saúde: como juntar os trapinhos?. História, Ciências, Saúde-Manguinhos, 9(2), 291-314.
CrossRef - Wallace, C. L., Wladkowski, S. P., Gibson, A., & White, P. (2020). Grief during the COVID-19 pandemic: considerations for palliative care providers. Journal of Pain & Symptom Management, 60,70-76. https://doi.org/10.1016/j.jpainsymman.2020.04.012
CrossRef - Weaver, M. S., & Wiener, L. (2020). Applying palliative care principles to communicate with children about COVID-19. Journal of Pain & Symptom Management. 60, 8-11. https://doi.org/10.1016/j.jpainsymman.2020.03.020
CrossRef - Fischer, M. L., Cunha, T., Renk, V., Sganzerla, A., & Santos, J. Z. D. (2017). Da ética ambiental à bioética ambiental: antecedentes, trajetórias e perspectivas. História, Ciências, Saúde-Manguinhos, 24(2), 391-409.
CrossRef - Fischer, M.L., Rosaneli, C.F., Cunha, T.R., Sganzerla, A., Molinari, R.N., & de Amorim Cini, R. (2018). Comunicações sobre a crise hídrica: a Internet como ferramenta de sensibilização ética. Sustentabilidade em Debate, 9(1), 158-171.
CrossRef - Barbosa, E. & Granado, A. (2004). Weblogs – Diário de Bordo. Porto: Porto Editora.
- Woodward, K. (2007). Identidade e diferença: Uma introdução teórica e conceitual. Petrópolis: Vozes.
- Minerbo, M. (1993). Intimidade e formas de intimidade: da escuta à teorização. Revista Brasileira de Psicanálise, 27(2), 223-48.
- Bauman, Z. (2004). Amor Líquido: sobre a fragilidade dos laços humanos. Rio de Janeiro: Zahar.
- Farias, L. & Monteiro, T. (2012). A identidade adquirida nas redes sociais através do conceito de persona. XIX Prêmio Expocom. http://www.intercom.org.br/papers/regionais/nordeste2012/resumos/r32-1497-1.pdf.
- Moretti, F. A., Oliveira, V. E. D., & Silva, E.M.K.D. (2012). Acesso a informações de saúde na internet: uma questão de saúde pública?. Revista da Associação Médica Brasileira, 58(6), 650-658.
CrossRef









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}